Varicose Veins
Varicose veins are defined as veins that are more than 3mm in diameter, and are usually palpable.
What causes Varicose Veins?
Varicose veins are a genetic condition. The actual cause is related to a change in the ratio of elastin and collagen in a vein wall. Hormones may influence the progression of veins in some individuals. Smoking, obesity and standing professions may aggravate veins.
Importantly, we are currently not able to cure or prevent veins – we treat problematic veins and then veins require ongoing maintenance.
Veins in the leg transport blood back to the heart, against gravity, and to prevent backflow there are valves within the veins. If these valves do not work there is ‘backflow’ of blood which distends the veins resulting in varicose veins, fluid retention and other symptoms.
This increased pressure is known as venous hypertension. As the pressure increases, these veins become more dilated and subsequently become visible as ‘varicose veins’.
In more advanced cases, swelling may result causing inflammation and damage to the skin. This can be seen as hardened dark skin, eczema and wounds may occur which are difficult to manage. Thus, one needs to optimally manage and maintain vein health.
Symptoms of Varicose Veins
Common symptoms of varicose veins include leg pain, swollen ankles and feet, itching, heavy legs, tired and aching legs especially towards the end of the day or after prolonged periods of standing or sitting.
Varicose Veins Treatment
The treatment of varicose veins has advanced significantly over the past couple of decades. Traditional treatment was invasive surgery that involved vein stripping with long recovery periods.
There are now minimally invasive techniques that treat veins and can mostly be done out of main theatre, under local anaesthetic and without the need for skin incisions or sutures.
How do we investigate veins?
Varicose veins are usually only the tip of the ice berg and are linked to deeper veins which may be causing the pressure on them. In order to get the full picture, we need to do a venous duplex doppler and vein map.
Ultrasound Mapping
An ultrasound investigation is a form of imaging that uses sound waves to formulate images. It is the same investigation that is used to monitor a baby in pregnancy. It carries no risk to the patient and is not painful.
An image is created of the blood vessels and valves within the vein, plaque in arteries, thrombosis and other diseases can all be seen. Colour can be used to help look at the blood flow in vessels and assess disease.
Vascular ultrasound has the additional element of ‘doppler’ which enables the type of flow in the blood vessels to be assessed to determine whether there is disease or not.
A probe is used at the site of investigation of the legs, neck and abdomen. Gel is applied so that a clear image can be produced. If you are having a Venous Duplex Doppler of the lower limbs, you need to be prepared that a proper investigation like this takes some time – between 30-45 minutes.
You will be required to lie down and to stand as the deep veins and superficial veins need to be assessed. Disease can occur along all aspects of the vein and thus the entire venous system needs to be assessed if a proper assessment and treatment is to be performed. Your legs will be scanned from the feet to the groin, from both the front and from behind.
In vein pathology, it is vitally important to have proper vein mapping done in order to target the problem veins and assess what is happening in all layers of veins and identify where varicose veins are linked to.
It also helps with vein maintenance as we will have a baseline map for you to monitor any changes.
Treatments Surgical:
Vein Stripping
The traditional surgical management of treating veins was vein stripping. This is an a operation that requires hospital admission and a general anaesthetic. An incision is made in the groin and at the knee and the long vein stripped out with resultant wounds. Recovery is more prolonged than current management. Endovenous techniques have taken over surgery as the gold standard. Vein stripping is rather outdated and hardly ever performed anymore - only in very select cases.
Endovenous Treatments
Thermal Ablation
- RadioFrequency Ablation
- Laser
Non-Thermal Ablation
- Mechano-chemical Ablation (MOCCA, Clarivein)
- Veneseal Ablation
Endovenous Ablation
The traditional treatment of treating a refluxing vein entailed surgery and ‘vein stripping’ or removal of the vein. This required hospital admission and a general anaesthetic. Surgical incisions are then made in the groin and at the knee and the offending vein is literally stripped out. The body is then able to use the deep venous system to return blood to the heart.
This is done under general anaesthetic, requires hospital admission and, although still may have a role in the individual patient, has generally been replaced with newer, quicker, less invasive and more pain-free techniques.
Endovenous treatments have replaced vein stripping. It is important to realise that varicose veins are branches off deeper veins. The deeper veins (saphenous veins) can usually not be seen and these are long veins running from the inside of the ankle to the groin, or the outside ankle to behind the knee – these veins are like tree trunks with varicose veins coming to the surface as branches, and thus it is only the edge of the branches that one sees at the skin.
Thermal Ablation: Radiofrequency (RFA) and Laser
Thermal treatments use minimally invasive technology to treat venous disease that has now largely replaced traditional surgery. This is done under local anaesthesia and patients can go home the same day. No hospital admission is required. Patients can return to normal daily activities by the next day.
Today we have the option of Endovenous Techniques, the thermal ones including Radio Frequency Ablation and Laser.
Radiofrequency ablation and Laser are minimally invasive treatments for varicose veins that use energy to heat and damage the walls inside the affected vein and cause them to seal off. This essentially closes off the problematic vein and directs blood to veins that are working normally. This is done under ultrasound guidance with a small catheter (thin tube) that goes inside the veins.
These are procedures that also address the refluxing veins with the same outcomes as surgery however they generally
- do not require hospital admission (unless there are combination procedures)
- do not require a general anaesthetic
- do not require surgical incisions to address the vein
- allow the patient to go home the same day
- allow the patient to return to normal activities the same day
- decreases pain and discomfort post procedure
There have been 4 randomised controlled trials comparing RFA to open surgery and RFA was significantly better in all of the following:
- less post-operative pain
- quicker recovery
- higher quality of life scores
- less bruising
Patients who underwent RFA were able to return to work more than one week earlier than those who underwent surgery. Eighty one percent of patients who underwent the RFA procedure returned to normal activities within one day whereas only 47% of those who underwent surgery were able to do this.
To view how the RadioFrequency procedure is done, Click Here.
Non-Thermal Endovenous Treatments
Mechano-Chemical Ablation (Clarivein)
Mechanochemical ablation is another endovenous technique used to treat damaged veins. This is a thin catheter that spins inside the vein irritating the inner lining of the vein wall and it sprays a sclerosant to seal the vein off. It does not use any heat. The advantage of this is that the catheter can be used right down to the ankle, which cannot be done with thermal treatments.
To see how the procedure is done: Click Here
Veneseal (Glue) Ablation
Veneseal is also an endovenous procedure and boasts little pain, no sclerosant and no need for compression. Veneseal is also a non-thermal endovenous technique, with the advantage of being able to treat right down to the ankle. The veins that are not working are sealed off by injecting a glue inside them. Another advantage is that there is reduced need for compression stockings.
For more information on the Veneseal, Click Here to watch.
Are endovenous treatments painful?
The only painful part is getting access to the vein, which is like having a drip.
In thermal endovenous treatments cold anaesthetic fluid (Tumescent) is also injected along the vein the RadioFrequency or laser will treat in order to protect the skin. During the clarivein procedure, one may be aware of the catheter in the vein (especially if the vein is near the skin), however, most patients describe it as a ‘buzzing’ or ‘vibrating’ sensation. If one is having additional treatment like phlebectomies of removal of varicose branches, local anaesthetic will be given.
Are there complications?
All endovenous procedures are considered low risk procedures and are generally safe. However, as we are working in the blood vessels and near the deep veins, there is a small risk of deep vein thrombosis. The procedures are always done under ultrasound guidance and measurements are performed in order to prevent proximity to the deep veins. You will always undergo a scan within the next week to assess the deep veins. The sclerosant that is used to seal the vein may cause some pigmentation along the vein. This will resolve in most people (only permanent in 1%) over a few months. Some patients may experience some numbness or hypersensitivity from nerve irritation. This will usually resolve over time, and permanent change only occurs in around 1% of patients.
Ambulatory Phlebectomy
Surface varicose veins are branches or tributaries of the deeper veins – they are representative of the tip of the iceberg to an entire deeper venous system that cannot always be seen. It is the deeper system that is treated with endovenous techniques such as laser or radiofrequency (and that was traditionally stripped out).
The varicose veins that are visible, are branches off these long veins, so they also need to be treated in order for them to disappear. They are too close to the skin and too tortuous for laser or radiofrequency, and we treat them by injecting ultrasound guided foam sclerotherapy with or without the addition of a technique called microphlebectomy (or ambulatory phlebectomy).
If they are very small they may just require ultrasound guided foam sclerotherapy (Ultrasound Guided Foam Sclerotherapy).
Microphlebectomy refers to removal of the varicose branch. It is not vein stripping.
In this procedure, varicose veins are marked pre-operatively and local anaesthetic is given. Tiny incisions are made and the branch is disconnected, or some of the branch may be removed. The incisions are tiny and no stitches are necessary. There will be some bruising and feeling of ‘lumpiness’ as it bled into the tissue, but this will go with time. It is necessary to do this to larger branches in order to get the leg flat and smooth in these areas. Foam alone will result in hard lumps, or the possibility of the veins re-opening.
What does the treatment involve?
The varicose veins that will be removed are marked whilst you are standing. You will then lie down and the leg will be cleaned and prepared in a sterile fashion. If an endovenous procedure is being performed, this will be done first. Local anaesthetic is injected into the skin over the varicose vein using a very fine needle. A tiny incision is then made and the vein is disrupted as part of it is removed. Depending on the size of the vein, the vein may be tied off. The incision will then be dressed with a plaster. A compression bandage will be placed around the leg for a period of 24 hours.
Ultrasound Guided Foam Sclerotherapy
Foam sclerotherapy is another modality to treat veins. It uses the same chemical as injection sclerotherapy but is made into a foam consisting of micro bubbles. The bubbles allow the sclerosant to sit on the surface of the bubbles and come in direct contact with the vein wall. Foam also travels well in veins and can be seen on ultrasound.
It is utilized for larger veins.
It has been previously shown to be inferior to surgical techniques in comparison but can be used as an adjunct for endovenous procedures, where catheter ablations are not technically possible and around ulcerations.
Foam travels well around ulcerations and can be tracked and followed up with ultrasound to aid in healing and reduce recurrence.
Excellent results can, however, be achieved if patients are followed up as sometimes additional injections are required. We have a set protocol for this to ensure optimal outcomes using foam.
Foam can be used in varicose branches that are visible but not large. This may reduce the need for small incisions to remove veins. However, it needs to be weighed up against the chance of the vein re-opening or a lump being felt (thrombosed vein).
For maintaining veins, annual scans are done comparing one’s original vein map – should any new problematic vein be identified, a foam injection can often halt the process and reduce the need for a repeat surgical intervention.



Varicose Veins

Ultrasound scan
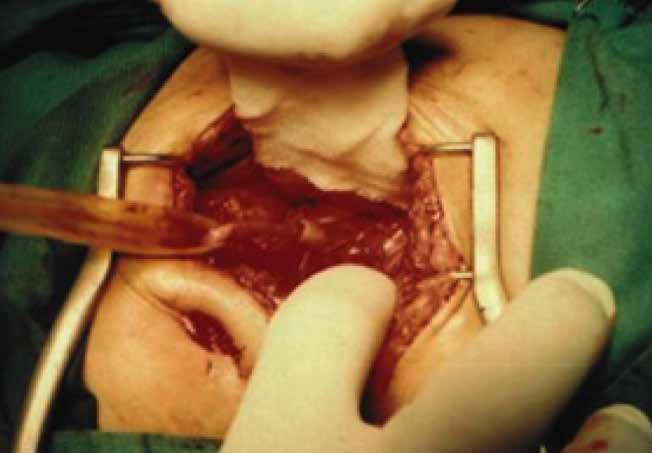
An incision is made in the groin to identify the Great Saphenous Vein..

Great Saphenous Vein stripped out from groin to knee.

Incision closed with stitches where the vein was stripped out.


Radiofrequency Ablation

Non-thermal Endovenous treatment: Mechano- Chemical Ablation (Clarivein)

Non-thermal Endovenous treatment: Veneseal (Glue) Ablation




Do you want to visit our clinic?
